Posted
10th July 2015
Research
A study from New York reports a reduction in C. difficile infection associated with the introduction of a pulsed-xenon UV (PX-UV) device. The authors performed a before-after study of the impact of adding PX-UV to the terminal disinfection protocol of rooms housing patients requiring contact precautions, with 12 months before and 12 months after implementation. Overall, there was a non-significant 22% reduction in the rate of CDI (from 1.06 to 0.83 cases per 1000 patient days), and a significant 70% reduction in the ICU (from 1.83 to 0.55 cases per 1000 patient days).
The authors note a change in cleaning contractor towards the end of the pre-intervention period, which could be a confounding factor. And a change in paediatric case mix, which may explain the marginal increase in CDI rates in paediatrics. More importantly, there is a comment in the discussion intimating that PCR testing may have been implemented during the study period, which would be a much more important confounder – but it is not clear whether PCR testing was implemented in the study hospitals or surrounding hospitals.
The authors introduce an unfortunate new term into the literature: “UVD” (ultraviolet light for room decontamination). This is used by the authors as a “catch-all” term to encompass both ultraviolet-C (UVC) and pulsed-xenon UV (PX-UV) devices. This is unfortunate because a recent study shows that a UVC device was, photon for photon, more effective than a PX-UV device.
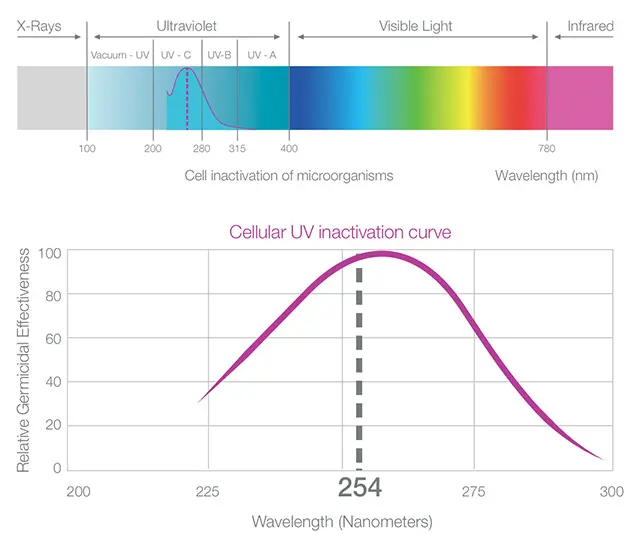
In the discussion, the authors comment that “Mercury bulbs emit a continuous low pressure light at a single range of 254 nm, and the effect of this UV light is cumulative requiring a longer cycle time of approximately 45 minutes for spore reduction.” Whilst the recommended cycle times for UVC devices are indeed longer than for PX-UV to address contamination with spores, the head-to-head study showed that UVC is more effective than PX-UV when run for the same length of time from the same point in the room. Put another way, a short blast of UVC would do more damage to spores than the same short blast of PX-UV. In the case of this study, if a UVC device had been run as per the PX-UV device, you’d expect to see more of an impact on the spores – and possibly more of an impact on CDI transmission.
The authors also comment that “Pulsed xenon devices also are somewhat safer because mercury-based devices can release toxic gases if they break accidentally.” This issue has been stirred up by manufacturers of PX-UV devices. The amount of mercury in the bulbs is tiny, and there are fail-safe systems in place to ensure that no mercury is released in the event of breakage. The truth is that a fluorescent bulb that you would see in an office block is more hazardous than the bulbs in UVC devices!
So, it seems that in line with other studies, augmenting terminal disinfection with a UV device does reduce C. difficile transmission. But there does not seem to be a good reason to choose PX-UV over a UVC device!
SHARE THIS ARTICLE
Tags
Latest News

Embracing sustainability and cost savings: The journey of Clinell Indicator Notes to paper-based solutions
At GAMA Healthcare, we’ve always prided ourselves on being at…

Introducing HEXI HUB: A seamless transition in our product line
We’re pleased to announce an update to our product offering…

Innovative solutions for tackling Carbapenemase-producing Enterobacteriaceae (CPE) at King’s College Hospitals
King’s College Hospital NHS Foundation Trust, one of London’s largest…

Gloves Off: reducing unnecessary plastic waste during environmental cleaning and disinfection
In this blog, Dr Phil Norville discusses the momentum-gaining ‘Gloves…